

Read our white paper, detailing the scope, extent and methodology of our research study with the University of Salford. You can read the full white paper here and download the PDF.
The use of Personal Electronic Devices (PEDs) by children and adolescents has rapidly increased over the last decade (Ofcom, 2017). Many fear that this may lead to increased musculoskeletal (MSK) risk. However, the evidence for this assumption is sparse. For the adult population, repeated studies have identified the link between the use of smartphones and tablets and the identification of risks factors associated with MSK pain. This project intends to identify the risk factors associated with MSK pain for under 18-year olds.
This white paper considers the recent evidence base related to the risk factors associated with technology use in children and explores what this could mean for industry in the future.
This white paper outlines:
- Why we are conducting research in this area, including key statistics
- The current evidence surrounding the relationship between MSK pain and discomfort in children and the use of PEDs
- What we are doing about the problem and the nature of the research
- How children use PEDs and the potential of them developing MSK pain or discomfort and what does that mean for industry in the future?
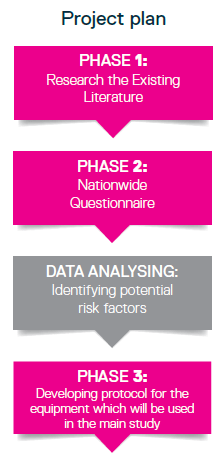
The research is to be conducted in 4 phases:
- Reviewing the existing literature and a systematic review will be published from the results
- A nationwide online questionnaire targeting 7-17-year olds, which will explore their PED usage and any muscle pain they are experiencing
- A pilot study to test equipment protocols, which will subsequently be used in the main study (phase four).
- A large-scale study designed to observe children's use of PEDs, then use research related devices to measure the children's posture. It is hoped that this will then allow us to identify potential risk factors for industry to consider regarding musculoskeletal pain in young adults joining the workforce.
The Need for Research into the Impact of PEDs on Musculoskeletal Signs and Symptoms and What We Know So Far
At some time in their lives a large percentage of the adult population experiences musculoskeletal disorders (MSDs) (Picavet and Hazes, 2003). Linked to this work-related musculoskeletal disorders (WMSDs) have increased over the last 10 years and it has been suggested that this is due to the rapid development and the use of computers by employees (Ulusam et al., 2015, Robertson et al., 2013, Piranveyseh et al., 2016, Ardahan et al., 2016).
However, to date there has been little research undertaken on risk factors related to children's use of personal electronic devices (including desktop computers, laptops, game consoles, mobile phones, and tablets) and whether there is any relationship between this usage and MSK pain and discomfort of children. However, there are a number of studies that have linked adult MSDs with the use of PEDs (Cho et al., 2012; Celik et al., 2018, Gerard et al., 2018). Therefore, much of the rational for this research is built on the literature related to adult populations.
Musculoskeletal disorders can affect muscles, joints and tendons in all parts of the body (Campbell, 2017). The most common types of MSDs are lower back pain and neck pain (Lunan et al., 2018). To help to avoid the development of
WMSDs the main risk factors need to be identified.
Work-related musculoskeletal disorders (WMSDs) have increased over the last 10 years and it has been suggested that this is due to the rapid development and the use of computers by employees (Ulusam et al., 2015, Robertson et al., 2013, Piranveyseh et al., 2016, Ardahan et al., 2016).
Key Statistics for Musculoskeletal Disorders
469,000 Workers [are] suffering from WMSDs (new or long-standing) in 2017/18' (Health and Safety Executive, 2018, p.5) and 6.6 million working days were lost.
Within these days the most common MSDs reported are :
- Lower back pain (LBP; 40%)
- Neck, shoulder and wrist pain (42%)
- Lower limb injuries (18%)
Upper limb disorders account for around 2.6m of days lost, with back disorders around 2.2m of days lost and lower limb disorders 1.7m days lost.
An average of 14 days were lost each episode of work absence.
Ill health among working-age people costs the economy £100bn a year in sickness absence and costs employers £9bn a year (Department for Work and Pensions and Department of Health, 2016).
Key Statistics for Adults with MSDs in the Workforce
The Office of National Statistics (2017) estimated the following percentages of adults experiencing MSDs, such as back and joint pain.
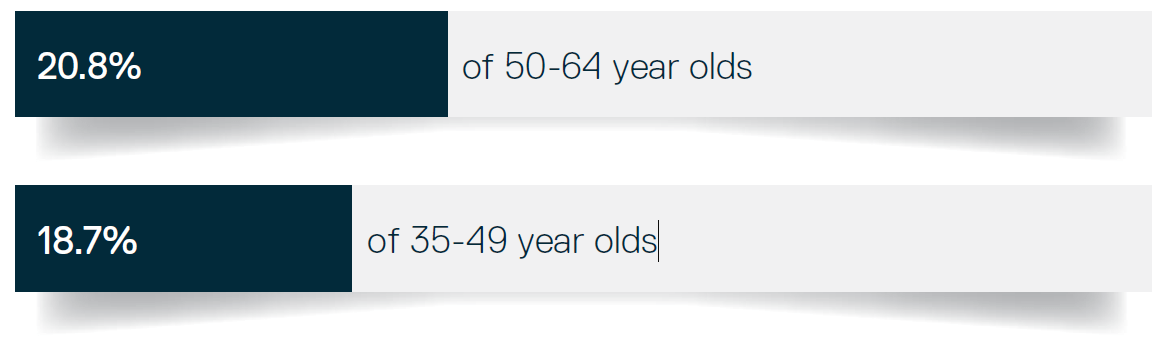
There are instances of younger adults entering the workplace with MSDs, but at present there is little research into musculoskeletal conditions and pain in children.
(Fares et al., 2017; Coleman Straker & Ciccarelli, 2009, Henschke et al., 2014).
In the USA, neck pain has been reported as the eighth most common disability pain for 15-19 year olds, with lower back pain being ranked the second (knee pain is ranked as the highest) (Inocencio, 2004; Kamper et al., 2016). It is also known that these musculoskeletal conditions may have a long-term impact in adolescents' working lives (Fares et al., 2017). With this in mind, it is important that there is a greater understanding of how and why musculoskeletal disorders first develop in children.
(Fares et al., 2017).
The Relationship Between MSDs and PEDs
There is a plethora of studies looking into the risk factors (e.g. amount of time using technology, type of technology being used and the position in which the participant is using the technology) associated with this increased use of technology and WMSDs
(Hossain et al., 2018; Celik et al., 2018, Wu, He, Li, Wang, & Wang, 2012).
Examples of WMSDs identified risk factors include:
Linked to this the following factors have been found to exacerbate to WMSDs: repetitive movements, gender and psychological stress.
Studies have linked musculoskeletal conditions in children to the use of PEDs identifying a combination of possible risk factors (e.g. type of PEDs, length of time using them, and how they are using PEDs) (Toh et al., 2017, Berolo et al., 2011, Sharan et al., 2014, Straker et al., 2008; 2010).
Laboratory studies found that awkward postures (increased neck flexion, lateral head tilt/rotation, trunk flexion/rotation), lack of movement and postural variation and altered muscle activity are all associated with computer use. However, these results need to be read with caution as the study was conducted in a laboratory and the results may differ if children were researched in their natural environment.
Currently, there is a lack of evidence looking at children in a more natural environment.
The Need to Look Earlier in the Life Course
Children have increased their use of technology, specifically PEDs and laptops/computers in recent times (Ofcom, 2016).
Key statistics for children increasingly using PEDs
In 2011-2012 98% of children between the ages of 10 and 15 used computers at home (The Office of National Statistics (ONS), 2014).
In England between 2006 – 2010, the proportion of children playing computer games for two hours or more at night increased from 42-55% in males and 14-20% in females (Public Health England, 2013).
An Ofcom (2017) online survey reported that:
- 12-15-year-olds
- 83% own their own smartphones and,
- 55% own their own tables
- 8-11-year-olds
- 39% own their own smartphones and,
- 52% own their own tablet
77% of 12-15 year olds reported playing video games for 12 hours per week and 99% go online for up to 12 hours per week (Ofcom, 2017).
However, there was a slight decrease in children using a computer to connect to the internet between 2009 -2010 (93%) to 2011-2012 (90%); this is hypothesised to be due to the increase of the use of PEDs over the computer (ONS, 2014).
A third of adolescents globally report musculoskeletal pain in some form on a regular basis (Kamper et al., 2016). Although the long-lasting effects of children having musculoskeletal conditions are not well researched, it has been suggested that musculoskeletal conditions in childhood may have long-reaching impacts into adulthood and the working population (Fares et al., 2017).
What is Known About Children Using PEDs?
- There is limited evidence that children’s usage of PEDs (how/where and duration) is a risk factor associated with MSK conditions. This limitation is due to the lack of/or low quality experimental, case-controlled and longitudinal studies.
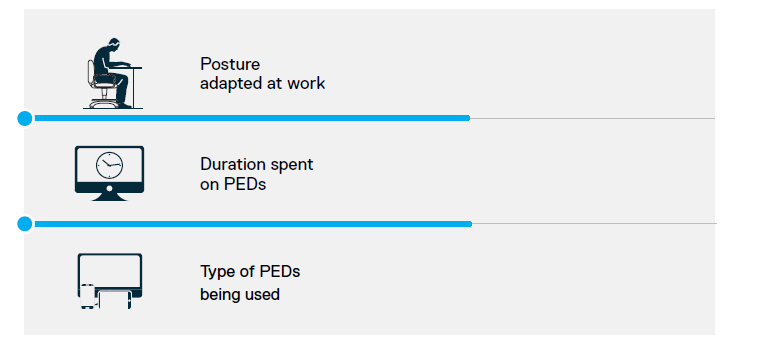
- The current evidence base suggests the risk factors of children using PEDs and developing MDS are the same as adults; duration spent on the device, type of device, and position adopted.
However, there are potentially other risk factors which, to our knowledge, have not been researched, although they have been found to impact adults, these are: repetitive use, positioning of PEDs and ergonomics, and support and/or position of the PEDS (with the use of accessories).
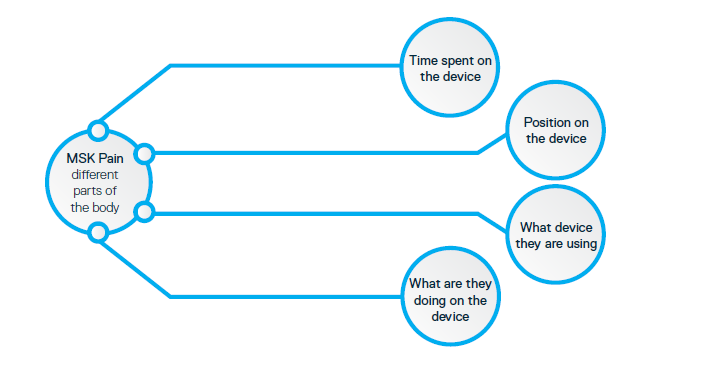
Some of the key influencing factors to take into account when thinking about MSK and PEDs are:
At present we do not know much about children's MSDs and if they are linked to PED usage. However, with the growing popularity of PEDs there is a real and urgent need to investigate this issue and find potential risk factors for children developing MSDs.
What is This Partnership Aiming to do About This Problem?
 In 2013 Cardinus Risk Management were made aware of a growing trend in the levels of discomfort school children were experiencing and the possible connection this could have with posture and increased technology usage among younger generations. In fact, there is a growing problem were children are developing injuries during their developmental years that could be major problems for them now and in the future workplace.
In 2013 Cardinus Risk Management were made aware of a growing trend in the levels of discomfort school children were experiencing and the possible connection this could have with posture and increased technology usage among younger generations. In fact, there is a growing problem were children are developing injuries during their developmental years that could be major problems for them now and in the future workplace.
This caused Cardinus Risk Management to start wondering about their clients' needs and what they might face in the future when a generation of children brought up using technology enters the workforce with pre-existing MSK conditions. As such they set out to understand:
What will be the effect on future employers of how children are using technology during their developmental years? Additionally, how will employers need to adapt to accommodate them?
Step 1:
As the first step of the research, a systematic review has been conducted. Looking at children's use of PEDs and the link to MSK pain. From there view it suggested that potential risk factors for children developing MSK pain when using PEDs are: 
– Duration spent on the device
– Type of device
– Position adapted
What did the literature search tell us?
- 43 relevant articles were found (after a systematic search of the literature and
screening) - No studies were conducted in England, the majority were conducted in Australia,
Brazil, South Africa or in the USA. Three of the studies were conducted in Ireland.
And the remaining 12 studies in European countries, China, Japan, Taiwan and Lebanon. - 28 out of the 43 studies looked at computer usage and only 6 looked at mobile phone usage (the other studies looked a combinations of technology)
- The age range of the studies was 3-18 years but commonly looked at 7-17 years
- 31 out of the 43 studies recorded MSK pain/symptoms using self-reported questionnaires and 8 used visual analogue scale and/or body discomfort chart
- Sixteen studies looked at the participant's posture
The Gaps in the Evidence Base that Were Identified From the Literature Search
More research is required into what technology children are using, how they are using it, where are they using it, the length of time they are using the device for and if they are experiencing any pain – at present, there is a big gap in the literature.
Step 2: Nationwide Online Survey
The focus of this phase will be to explore, through a nationwide online questionnaire, how children (between the ages of 7-17) report their use of PEDs, for example: what device they use, how often they use them, where they use them, how long they are on them and what position they are in when using them, and their self-reported MSK pain.
This will be done via a social media campaign targeted at schools, press releases and using Cardinus' clients and their connections.
The questions will include:
- What PEDs they use
- How often they use the PEDs
- What position they use the device in e.g. sitting, lying, etc.
- What are they doing on the device e.g. games, homework, social media
- At what age they started using PEDs
- Are they experiencing any MSK pain?
From the results of this questionnaire, we will have a better idea of how children are using devices and any related risk factors or MSD.
Step 3: Protocol Development
This phase will be a small pilot study to determine how to objectively measure the different biomechanical/physiological risk factors with a mobile laboratory (which can be taken into a school/homes). Step 3 will develop and test a protocol comprising of different equipment/devices that enable the measurement of biomechanical/physiological elements such as postural changes and increases in muscle activity that may be associated with PED usage and risk factors.
The portable equipment will be tested and compared to equipment that can only be used statically in laboratory settings for accuracy, validity and reliability to use in schools and homes.
Step 4: Physical Observations and Joint Movement/Measurements Taken
Phase four will involve a large-scale study designed to observe children's use of PEDs, using equipment and protocols to measure the children's posture as well as a subjective questionnaire. This will, in turn, allow us to identify potential risk factors for industry to consider regarding musculoskeletal pain that has developed in young adults joining the workforce.
From analysing the data which will be obtained we will be able to:
- Identify potential risk factors of children developing MSDs from using PEDs
- Consider what this means for industry in the future
- Identify future research avenues
Conclusions
It is notable that there is an increase usage of PEDs by children. Currently there is limited research conducted on the effects on children's MSK pain and the usage of PEDs. However, there is a plethora of evidence looking at adults and their usage of PEDs, but it is now time to focus on the next generation of PEDS users, children and adolescents.
We know that there is an increase in children using PEDs and that children are commonly complaining of back and neck pain, but what we don't know is if these are linked. The proposed research will help to identify if there is a correlation.
From an industrial point of view, doing this research will enable companies to prepare for the future workforce using the knowledge they have of potential risk factors. With a better understanding of MSK pain and more preparations in place, this will hopefully reduce the number of sick days within the future workforce, having a positive impact on the economy.
From the proposed research outlined it is hoped we will understand:
- If the increase of children's usage of PEDs is affecting their posture and MSK conditions
- If there are any identifiable risk factors of children developing any MSK conditions
- And prepare for the future workforce using the knowledge they have of potential risk factors
This white paper was put together by our PhD student, Anna Clark. Download the full PDF here.
CLICK HERE TO DOWNLOAD THE WHITE PAPER
{kind=link}